Researchers in the Biomechanics Group, in collaboration with the Department of Clinical Neurosciences, have gained deeper understanding into the mechanics of the skull that can lead to better ways to treat patients with traumatic brain injuries.
In theory the larger the amount of skull removed the better it will relax the pressure and you’ll get smaller regions of damage.
Michael Sutcliffe
A paper, published recently in Annals of Biomedical Engineering, explores some of the clinical issues surrounding decompressive craniectomy. Patients who have suffered traumatic injuries to the head, are victims of stroke or are experiencing a number of other illnesses or infections might undergo severe swelling of the brain. The worry is that, left alone, intracranial pressure can build and permanently damage the brain.
In a decompressive craniectomy, parts of the skull are removed surgically with the goal of allowing the brain to swell without causing damage. This procedure is not without controversy and it is still something of an open question as to how the operation can be optimised to lead to the most positive outcomes for the patient.
To tackle this problem, a cross-disciplinary team of Cambridge researchers wanted to model just how a craniectomy affects the brain. The work was a collaboration between a team led by Dr Michael Sutcliffe, Head of the Biomechanics Group, and a team from the Division of Neurosurgery at Addenbrooke’s Hospital that included Professor Peter Hutchinson (Professor of Neurosurgery), Dr Angelos Kolias (Clinical Lecturer in Neurosurgery), and Hadie Adams (Clinical Research Fellow).
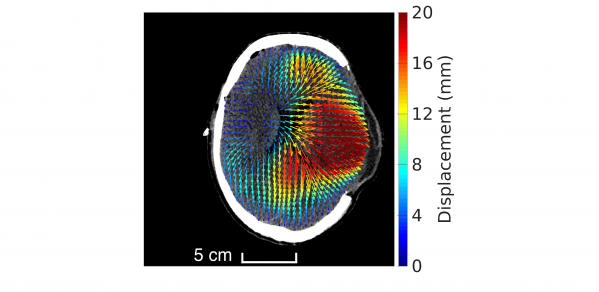
The engineering approach to craniectomy included looking at how to balance the trade-off between the size of the hole in the skull and the shear strain in the brain.
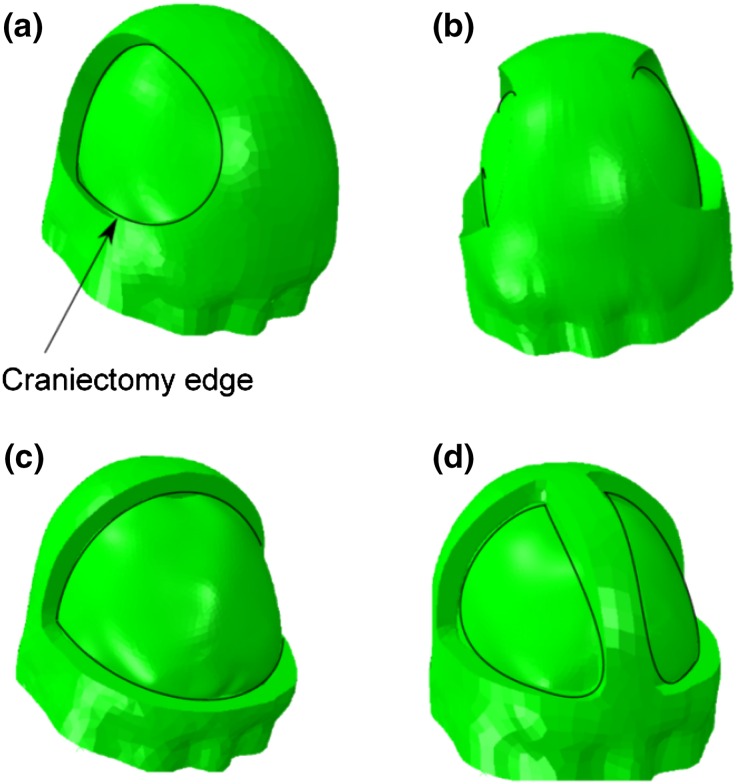 Examples of different craniectomy geometries
Examples of different craniectomy geometries
“This trade-off means that in theory the bigger you make the hole the better it will relax the pressure and you’ll get smaller regions of damage,” Dr Sutcliffe said. “But this has side-effects associated with it in the sense that if you have a bigger hole you might get an infection or it might be more difficult to reconstruct the skull.”
To find the right balance, Dr Sutcliffe’s team considered different sizes of holes to try to discover an optimal point where a further increase in the size of the skull opening no longer gave any benefits in terms of reduced damage. “Imagine if you took out half the skull – that would be unreasonable clinically,” Dr Sutcliffe said. “But our modelling offers some guidelines and helps understand how large a part of the skull should be removed to avoid undesirable side effects.”
According to Dr Kolias, bioengineering approaches such as the one described in the paper can help neuroscientists better understand the effects of craniectomy on brain tissue. This work is related to recently published results of a 10-year-long RESCUEicp trial that examined the role of craniectomy as a last-tier therapy for head-injured patients with refractory intracranial hypertension.
“The results confirmed the life-saving nature of the operation,” Dr Kolias said. “However, the outcomes of survivors ranged from vegetative state through varying states of disability to good recovery. Hence, there is a real need to understand the factors that could affect the outcome of patients following craniectomy.
“A multidisciplinary approach to the issue of brain deformation following craniectomy will play a central role in the efforts to optimise patient outcomes,” Dr Kolias said.
Modelling of Brain Deformation After Decompressive Craniectomy: https://dx.doi.org/10.1007/s10439-016-1666-7
